

Ah . . . the VMO, the Holy Grail of treating patellofemoral pain syndrome (PFPS). Shortly before I began the physical therapy program at UNMC, one of my professors and mentors published a study in our professional journal, Physical Therapy; their findings “do not support the notion that concurrent use of the hip adductors during knee extensor exercises results in preferential strengthening of the VMO.” That was in 1993. And yet, practitioners continue to prescribe exercises hip adductor/knee extension combination exercises for patients diagnosed with PFPS. These two videos purport to show just how to do it . . . yes, both involve squeezing a ball between the knees!
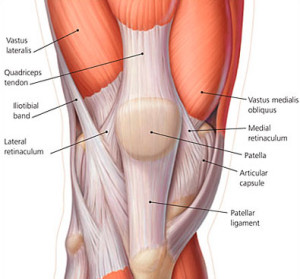 What is the VMO, anyway? The VMO is a collection of muscle fibers from the vastus medialis that run more horizontally than the other portions of this muscle. It has been theorized that because these muscle fibers are aligned in this way, they can pull the patella medially/inward to reduce any poor alignment or movement problems the patella might have (i.e., lateral tilt or glide). To be sure, an a priori analysis would suggest that strengthening the VMO would do what many say it does.
What is the VMO, anyway? The VMO is a collection of muscle fibers from the vastus medialis that run more horizontally than the other portions of this muscle. It has been theorized that because these muscle fibers are aligned in this way, they can pull the patella medially/inward to reduce any poor alignment or movement problems the patella might have (i.e., lateral tilt or glide). To be sure, an a priori analysis would suggest that strengthening the VMO would do what many say it does.
But it just can’t be done!
So, here is a list of reasons why we need to abandon the idea that exercises for PFPS should not be done with a ball between the knees in the hopes that strengthening the VMO will alleviate that pain.
To date, few, if any, well-executed, peer-reviewed research studies has shown that it is possible to isolate (AT ALL) the VMO. One of the modern-day PFPS “guru’s” just last week admitted that the VMO can NOT be preferentially targetd. So why do we still try?
Myth busting at #PFPManchester ‘can VMO be preferentially strengthened?’ Jenny McConnell says ‘no’ #busted
— Bill Vicenzino (@Bill_Vicenzino) September 5, 2015
Further, a study from August showed that it is not the VMO alone that atrophies (gets smaller and weaker), it is all the quadriceps. While the Australian researchers showed that all quadriceps decrease in size,
These findings suggest that atrophy is present in all portions of the quadriceps in individuals with PFP, and that exercises with the goal to preferentially activate and strengthen the VMO are not justified in this population.
So if it isn’t atrophied in the first place, why are we so desperate to perform isolated strengthening exercises for it?
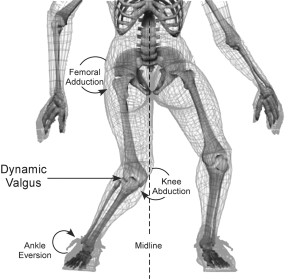 One position has been shown to contribute PFPS, dynamic valgus. Dynamic valgus is a moving measurement of the traditional Q-Angle (which has NOT been shown to contribute to PFPS) is a combination of hip/femoral adduction and hip/femoral internal rotation. It commonly occurs with a rapid increase in a person’s height, making control of the longer levers (bones and trunk) more difficult. That can be a challenge just walking up and down stairs. Now imagine increasing the impact, force, and velocity of sporting movements like running, sprinting, jumping, landing, or cutting; that abnormal position further exposes the athlete to stresses that contribute to PFPS.
One position has been shown to contribute PFPS, dynamic valgus. Dynamic valgus is a moving measurement of the traditional Q-Angle (which has NOT been shown to contribute to PFPS) is a combination of hip/femoral adduction and hip/femoral internal rotation. It commonly occurs with a rapid increase in a person’s height, making control of the longer levers (bones and trunk) more difficult. That can be a challenge just walking up and down stairs. Now imagine increasing the impact, force, and velocity of sporting movements like running, sprinting, jumping, landing, or cutting; that abnormal position further exposes the athlete to stresses that contribute to PFPS.
So, look at the dynamic valgus picture included here. one of the components of this position is hip or femoral adduction. What causes this movement?
- Weak hip abductors?
- Poor motor control?
- Habit?
- Improper instruction?
It certainly can be weakness in muscles that produce motion in the opposite direction (i.e., abduction). But I don’t know that we can definitively state that weak hip abductors cause this position and therefore PFPS; it is possible, but research is mixed, to be sure. (Check out this interesting article by Hewett and Myer‘s group for more info.) Another possibility is hip adductors that are too strong, though I have not seen research to indicate that is the case.
Simply put, the knee works best when moving in the sagittal plane as the muscles that absorb force and/or control the trunk, hip, and knee function are more efficient and better positioned to do so in the sagittal and not the frontal plane.
Given that, putting a ball between one’s knees does one of two things:
- Strengthens the hip adductors. If these are stronger, it seems the hip will adduct more during movement causing a position we don’t want (dynamic valgus).
- Encourages a position we don’t want by providing a stimulus to promote it. Stated differently, the ball between the knees encourages the person to press against the ball (think other manual therapies and the effect touch has); what happens when the ball is removed, the knees want to move against that same thing, resulting in the dynamic valgus position.
Lastly, to those that say, “but I have been doing this for years and it works,” my response. One of my mentors, strength training pioneer Tom Baechle, once told me that even if somebody lifts with poor technique, they are still lifting and will get stronger, but at what risk? The same applies here; PFPS treatment SHOULD include strengthening exercises and people will improve to a degree even when performing exercises with a ball between the knees . . . but at what risk to future injury?
So, if we can agree that . . .
- the VMO cannot be preferentially activated (1, 2),
- the VMO is not isolated in its weakness with PFPS (1),
- dynamic valgus increases the incidence of PFPS (1, 2, 3),
. . . why do an exercise that contributes to that position?